So you have a butt rash. We appreciate when patients behave well in the office, but sometimes it’s necessary for them to show the dermatologist their butts. We are over the moon to share with you 5 common skin problems found on a person’s backside (buttocks)!
Got a butt rash–or some other skin, hair or nail problem? Schedule an appointment with our board-certified dermatologist here!
Medically Reviewed by board-certified dermatologist Dr. Dina Strachan This content is for educational purposes only and is not a substitute for medical advice. We cut through the marketing hype to bring you products with proven active ingredients. Every item is reviewed by our clinical team for safety and efficacy—we strictly recommend products we would prescribe to our own patients.
Note: This content is for education and does not replace a medical evaluation. Aglow Dermatology may earn a commission if you purchase through our links, which supports our free educational content.
Genital herpes sometimes presents instead on the buttocks
1. Genital herpes
If you have been getting a recurrent sore on the exact same place on the buttocks, it would be a good idea to get screened for genital herpes. Genital herpes? On the buttocks?
After the primary infection with genital herpes, the virus lives dormant in the sacral ganglion in the lower spine. When the virus reactivates, it travels down the nerve toward the genitals—but sometimes takes an alternate route to the skin on a branch of the sacral nerve that serves the buttocks. This may cause a painful or itchy, recurrent butt rash.
Herpes is a lifelong infection. The good news is that over time people tend to have fewer outbreaks. Many people with genital herpes have no symptoms at all–but they can still infect others. Treatment is not always necessary. Treating genital herpes on the buttocks may include antivirals such as acyclovir, valacyclovir (Valtrex), or famacyclovir (Famvir). It’s important for pregnant women to let their obstetrician know if they have genital herpes to take measures to prevent infection of the baby during vaginal delivery.
If you have a recurring sore in the exact same spot, it isn’t a random rash—it’s likely the virus reactivating along the nerve.
When to See a Dermatologist for Genital Herpes
Seek Medical Guidance Early: If you suspect you have genital herpes, consult a professional to understand what to expect, get treatment and learn how to manage infection control.
Active Blisters or Open Sores: It is critical to see a provider while a sore is active; this is the only window of time to perform a viral culture or PCR swab for a definitive diagnosis.
Frequent Outbreaks: If you experience 4 or more outbreaks per year, seek medical advice to discuss daily suppressive therapy, which can significantly reduce the frequency of symptoms.
OTC Recommendations for herpes on the butt:
Pain Relief: Topical Lidocaine patches to numb the area during an outbreak.
Skin Protection:Hydrocolloid bandages tocover active sores, which prevents friction and reduces the risk of spreading the virus to other parts of the skin (autoinoculation).
Butt acne is sometimes like acne vulgaris that we get on our faces and sometimes different
2. Butt acne/folliculitis
“Butta face?” About 10% of people have a follicular papules on their buttocks–or butt acne. It’s not always exactly like the acne vulgaris we usually see on the face, which technically starts with microscopic white heads and black heads. Sometimes butt acne is a kind of irritant folliculitis caused by friction, sweat and bacteria. They both may respond to benzoyl peroxide wash, antiperspirants, or antibiotics.
When to see a Dermatologist for butt acne
See a dermatologist if the bumps become large, painful, and warm to the touch (signs of a boil or abscess) or if the eruption doesn’t clear. If your “acne” is leaving behind deep dark spots or scars, professional-grade topical or oral antibiotics may be necessary. And sometimes buttocks acne is a much more serious condition called hidradenitis suppurativa.
OTC Recommendations:
Benzoyl Peroxide 10% Wash. Use this in the shower, leave it on for 2 minutes, then rinse. It kills the bacteria that causes the inflammation. Rinse it off well as it can bleach towels, clothings and sheets.
Salicylic Acid Wash. If you are allergic, or not a fan of benzoyl peroxide, try a salicyclic acid acne wash instead. It unclogs pores and is antiinflammatory.
Antiperspirant. If sweat is the cause of your buttocks acne, antiperspirants can help reduce your breakouts.
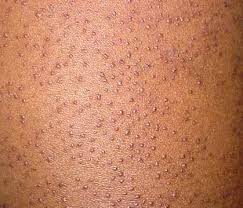
Those “chicken skin” bumps that we commonly see on the arms, back and thighs can also occur on the buttocks. They are caused by a buildup of keratin blocking the hair follicle. These lesions are a normal finding on some people. Sometimes people mistake keratosis pilaris for acne. It can be difficult to treat keratosis pilaris. Sometimes exfoliating creams, such as salicylic acid cream,ammonium lactate lotion, or physical exfoliation can make the skin smoother—but the effects are usually temporary. Keratosis pilaris is more common in people with eczema, or atopic dermatitis.
When to see a Dermatologist: KP is harmless, but if the bumps become intensely itchy, bright red, or don’t respond to any “rough and bumpy” lotions, a dermatologist can prescribe topical steroids for symptoms, higher-strength retinoids or discuss laser hair removal treatments.
OTC Recommendations:
Chemical Exfoliant:Ammonium Lactate (12%) Lotion or Urea Cream. These help dissolve the keratin plugs.
Smoothing Cream:Salicylic Acid Creams (SA). These provide a dual action of hydrating while gently exfoliating the skin surface.
Psoriasis is an autoimmune that characteristically involves the skin but that can affects joints and cardiovacular health. On the skin we tend to think of psoriasis as occuring on the elbows and knees. Psoriasis is among a variety of “red rashes” that dermatologists see that may look the same. Drug eruptions. Pityriasis rosacea. Syphilis. Pityriasis rubra pilaris…and psoriasis. Sometimes the key to distinguishing them is the presence of gluteal pinking, which is involvement of the fold between the cheeks of the buttocks.
Psoriasis in the gluteal fold (inverse psoriasis) can be tricky because it often lacks the typical “silvery scale” found on elbows.
When to see a Dermatologist: If you have a persistent, shiny red rash in the buttock fold that doesn’t respond to anti-fungal creams. If you know you have psoriasis, get under the care of a dermatologist for the long-term. Psoriasis is a systemic inflammatory condition; a dermatologist needs to evaluate you to prevent skin thinning and to check for associated joint pain (psoriatic arthritis) and heart disease. Treatments a dermatologist include:
topical medications such as steroids and others
oral and injected systemic medications such as biologics
Steroid-Free Relief:Coal Tar Gel or Psoriasis Medicated Washes.
Anti-inflammatory:Hydrocortisone 1% (no more than 1-2 weeks). Using hydrocortisone in folds can increase the risk of a fungal infection.
Mycosis fungoides- a types of skin cancer that sometimes presents as a butt rash.
5. Skin Cancer: Mycosis Fungoides/CTCL
Mycosis fungoides (MF), or cutaneous T-cell lymphoma (CTCL), is a relatively uncommon type of skin lymphoma that can look like eczema or psoriasis. This condition, versus sun-associated skin cancers, typically involves the “double covered” areas of the body that get less sun such as the breasts in women, as well as the hips and buttocks. This condition can persist for decades without changing life expectancy, but in some cases it is more aggressive causing sickness and death. Interestingly, unlike many other types of skin cancer, which more commonly occur in people with less pigmented skin, CTCL is more common in people with skin of color. If CTCL, or another type of skin cancer, is of concern, see a board-certified dermatologist for a skin cancer screening. Make sure you tell the doctor about your concern in the buttocks area as this isn’t always checked.
Remember: Mycosis Fungoides (MF) can masquerade as eczema or psoriasis for years.
When to see a Dermatologist:This requires an in-person visit. If you have a “rash” that has not moved or changed for months, or a patch of skin that feels thicker/scaly despite using moisturizers, you need a skin biopsy. Early detection of CTCL is critical for a normal life expectancy.
OTC Recommendations:
Note: There are no OTC “treatments” for skin cancer- see a dermatologist.
Supportive Care: While waiting for your appointment, use Fragrance-Free, Hypoallergenic Ointments (like Petrolatum) to soothe dry, scaly patches and prevent secondary irritation.
Conclusion: Butt Rashes
The butt is just another part of the body with skin. There is more to butt rashes than diaper rash. If you have a problem in this area, don’t be shy to show your dermatologist.